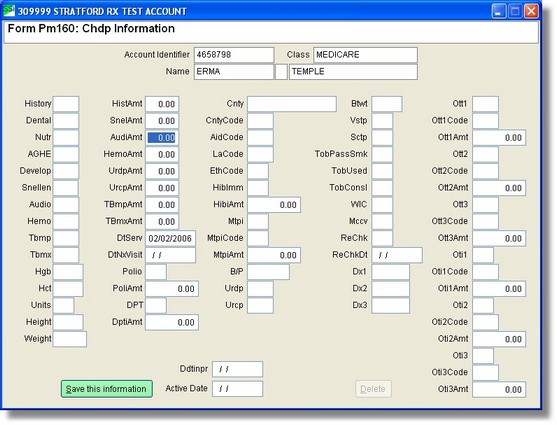
History
History and Physical Exam
Please enter history and physical exam result code
Please enter history and physical exam fee
Dental
Dental Assessment/Referral
Please enter dental assessment result code
Nutr
Nutritional Assessment
Please enter nutritional assessment result code
AGHE
Anticipatory Guidance Health Education
Please enter antic. guidance health dev result code
Develop
Developmental Assessment
Please enter developmental assessment result code
Snellen
Snellen or Equivalent
Please enter Snellen or equivalent result code
Please enter Snellen or equivalent fee
Audio
Audio metric
Please enter audio metric result code
Please enter audio metric fee
Hemo
Hemoglobin or Hematocrit
Please enter hemoglobin or hematocrit result code
Please enter hemoglobin or hematocrit fee
TB Mp 11
Tb Multipuncture
Please enter Tb Multipuncture result code
Please enter Tb Multipuncture fee
TB Mx 12
Tb Mantoux
Please enter Tb Mantoux result code
Please enter Tb Mantoux fee
The following screens apply to OtTst 13, 14, and 15
Other Tests
1 Sickle Cell (13)
2 Lead:FEP (14)
3 Lead:Blood (15)
4 VDRL/RPR/ART (16)
5 G.C. Culture (17)
6 Pap Smear (18)
7 PKU:Blood (19)
8 Chlamydia (20)
9 Pelvic Exam (21)
B Leave Blank
Result codes
A No Problem Suspected
B Refused or Not needed
C New Problem Suspected
D Known Problem
E Leave Blank
HGB 28
Hemoglobin
Please enter patient's hemoglobin
HCT 29
Hematocrit
Please enter patient's hematocrit
Units
<A>=Inch, Pound, Ounce Unit
<M>=Metric Unit
Please enter <A>=inch, pound, ounce unit <M>=metric units
Height
Height
Please enter patient's height
Weight
Weight
Please enter patient's weight
HistAmt
SnelAmt
AudiAmt
HemoAmt
UrdpAmt
UrcpAmt
TBmpAmt
TBmxAmt
DtServ
Date of Service
Please enter date of service
DtNxVisit
Next Visit
Please enter date of next visit
Polio
Immunization Results
A Given today/Up to date
B Given today/Not up to date
C Not given today/Up to date
D Refused or contra-indicated
E Leave Blank - No Answer
Please enter POLIO immunization status <A>,<B>,<C>,<D>, or <E>.
PoliAmt
DPT
Diphtheria, pertussis, tetanus
Immunization Results
A Given today/Up to date
B Given today/Not up to date
C Not given today/Up to date
D Refused or contra-indicated
E Leave Blank - No Answer
Please enter DPT immunization status <A>,<B>,<C>,<D>, or <E>.
DptiAmt
Cnty
County
Please enter patient's county of residence
CntyCode
AidCode
L.A. Code
L.A. Code
Please enter L.A. code
EthCode
Ethnic Code
Please enter patient's ethnic code
Ethnic Codes
1 Am. Indian
2 Asian
3 Black
4 Filipino
5 Hispanic
6 White
7 Other
8 Pacific Is
9 Leave Blank
HibImm
Immunization Results
A Given today/Up to date
B Given today/Not up to date
C Not given today/Up to date
D Refused or contra-indicated
E Leave Blank - No Answer
Please enter Hib Cv immunization status <A>,<B>,<C>,<D>, or <E>.
HibiAmt
Mtpi
MtpiCode
MtpiAmt
B/P
Blood Pressure
Please enter patient's blood pressure
Urdip
Urine Dipstick
Please enter urine dipstick result code
Please enter urine dipstick fee
Urcmp
Complete Urinalysis
Please enter complete urinalysis result code
Please enter complete urinalysis fee
BtWt
Birth Weight
Please enter patient's birth weight
Vstp
Sctp
TobPassSmk
Patient Exposed to Passive Smoke
Please enter Y/N is patient exposed to tobacco smoke?
TobUsed
Tobacco used by Patient
Please enter Y/N does the patient use tobacco?
TobConsl
Counseled About Tobacco Prevention?
Please enter Y/N was the patient referred for tobacco use counseling?
WIC
Please enter Y/N - was patient enrolled in WIC?
Mccv
ReChkDt
Screening Procedure Recheck
Please enter procedure recheck date
RchkDt
Dx1
Dx2
Dx3
Diagnosis Code
Please enter diagnosis code
Ott1, Ott1 Code, Ott1Amt
Other Immunization #1 Code
Immunization Type
1 Measles (34)
2 Mumps (35)
3 Rubella (36)
4 Hib (37)
5 Polio (IPV) (39)
6 Leave Blank - No answer
Please enter other immunization #1 code
Please enter the fee.
OtOtt2, Ott2 Code, Ott2Amt
Other Immunization #2 Code
Immunization Type
1 Measles (34)
2 Mumps (35)
3 Rubella (36)
4 Hib (37)
5 Polio (IPV) (39)
6 Leave Blank - No answer
Please enter other immunization #2 code
Please enter the fee.
Ott3, Ott3 Code, Ott3Amt
Other Immunization #3 Code
Immunization Type
1 Measles (34)
2 Mumps (35)
3 Rubella (36)
4 Hib (37)
5 Polio (IPV) (39)
6 Leave Blank - No answer
Please enter other immunization #3 code
Please enter the fee.
Oti1, Oti1 Code, Oti1Amt
Other Test #1
Please enter the number of the other test #1
Please enter the other test #1 result code
Please enter the other test #1 fee
Oti2, Oti2 Code, Oti2Amt
Other Test #2
Please enter the number of the other test #2
Please enter the other test #2 result code
Please enter the other test #2 fee
Oti3, Oti3 Code, Oti3Amt
Other Test #3
Please enter the number of the other test #3
Please enter the other test #3 result code
Please enter the other test #3 fee
InScr 39
Initial Screen
Please enter Y/N was this an initial screen?
PtlSc 45
Partial Screen
Please enter Y/N is this a partial screen?
Mcal 47
Covered by Medicaid
Please enter Y/N Is patient covered by Medi-Cal?
MMR 33
Measles, mumps, rubella
Immunization Results
A Given today/Up to date
B Given today/Not up to date
C Not given today/Up to date
D Refused or contra-indicated
E Leave Blank - No Answer
Please enter MMR/MuR/MB immunization status <A>,<B>,<C>,<D>, or <E>
Please enter the fee.
Immunization Type
1 MMR (measles/mumps/rubella)
2 MuR (mumps/rubella
3 MR (measles/rubella)
4 Leave Blank - No answer
Please enter MMR/MuR/MB immunization type 1,2,3,4.
Immunization Results
A Given today/Up to date
B Given today/Not up to date
C Not given today/Up to date
D Refused or contra-indicated
E Leave Blank - No Answer
RefTo 21
Referred to (first)
Please enter (first) person referred to
RefTo 22
Referred to (second)
Please enter (second) person referred to
Cmmts 23
Comments
A pop-up screen will appear which is labeled Enter Comments/Problems
Press [ESC] to quit without saving
Press [CTRL+W] to save your notes
NewPt 38
New Patient
Please enter Y/N was this a new patient or an extended visit?