Institutional billing specifications - set up the insurance claims.
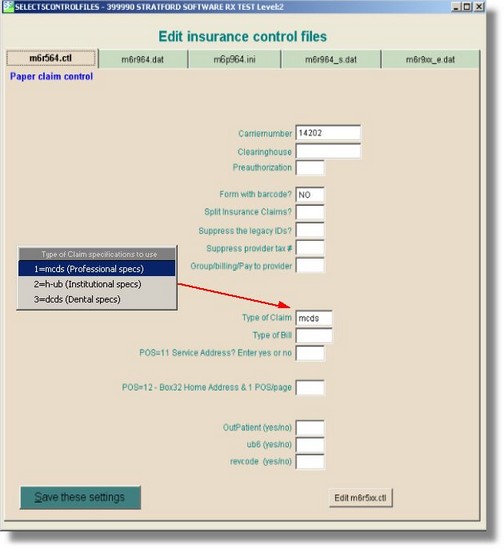
To set up a specific form type for UB04, from the main directory select #8, #7, #3 and then enter the form type: (example: 564/964) and then select the 1st tab for the paper claim information. Right click on the 'Type of Claim" text box and select 2=h-UB04 (institutional specs)
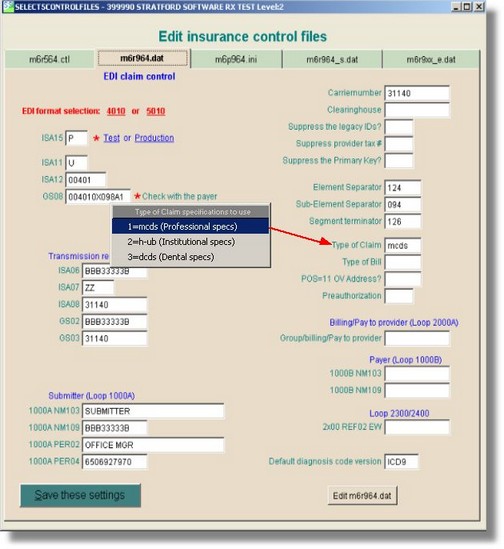
For 'UB04/Institutional' type EDI, select the 2nd tab for EDI information. Right click on the 'Type of Claim" text box and select 2=h-UB04 (institutional specs)
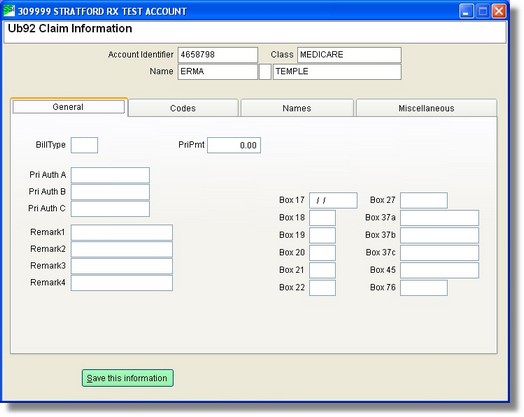
Next you need to go into the patient's account, enter the insurance and the select the UB04 claiim question screens below.
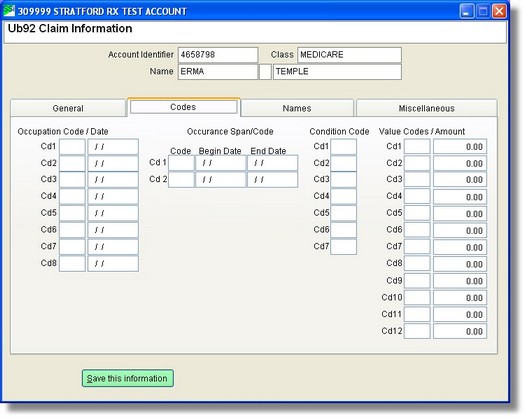
OccCd/Dt 01 02 03 04 05 06 07 08 09 10
Occurrence Code
Please enter 1st occurrence code
Please enter 1st occurrence date
Please enter 2nd occurrence code
Please enter 2nd occurrence date
Please enter 3rd occurrence code
Please enter 3rd occurrence date
Please enter 4th occurrence code
Please enter 4th occurrence date
Please enter 5th occurrence code
Please enter 5th occurrence date
CondCode 11 12 13 14 15
Condition Code
Please enter 1st condition code
Please enter 2nd condition code
Please enter 3rd condition code
Please enter 4th condition code
Please enter 5th condition code
Bld Furn 16
Blood Furnished
Please enter the number of units of blood furnished.
Bld Rpl 17
Blood Replaced
Please enter the number of units of blood replaced.
Not Rpl 18
Not Replaced
Please enter the number of units of blood not replaced.
Bld Ded 19
Blood Deductible
Please enter number of non replaced deductible units of blood supplied.
VaCd/Amt 20 21 22 23 24 25 26 27
Value Code
Please enter 1st value code.
Please enter 1st value amount.
Please enter 2nd value code.
Please enter 2nd value amount.
Please enter 3rd value code.
Please enter 3rd value amount.
Please enter 4th value code.
Please enter 4th value amount.
Deductbl 28
Deductible Amount
Please enter the cash and/or blood deductible amounts.
CoInsurn 29
Co-insurance Amount
Please enter amount collected from the patient toward the co-insurance.
Employee ID 30
Please enter employee ID number.
EmInData 31
Employment Information Data
Please enter employment information (enter ABCPSFM).
EmStCode 32
Employment Status Code
Please enter employee status code 1= Full-time 2= Part-time
EmLocatn 33
Employer Location
Please enter the specific employer location, the city, plant, etc.
Remarks 34 35 36
Please enter 1st remark line.
Please enter 2nd remark line.
Please enter 3rd remark line.
Bill Type 37
Please enter bill type.