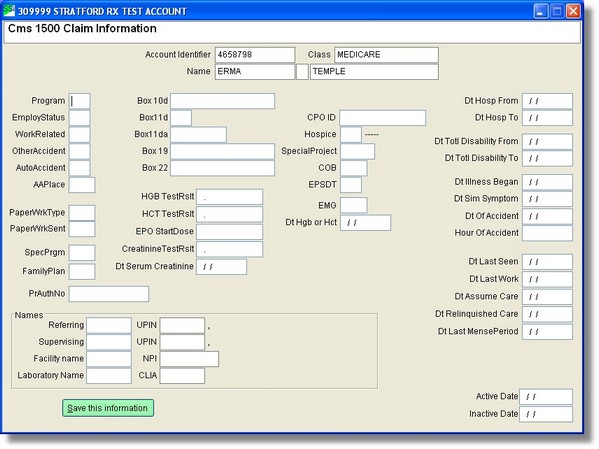
Many of the text boxes are for specialized billing. Do not use them unless you know for sure that you need them. Your best reference is the EDI specifications for your specialty.
Program
Applicable program
Type of Program (codes below are applicable to the EDI claim also)
12 MSP, working aged beneficiary
12 MSP, spouse w/employer GHP
13 MSP, ESRD beneficiary 12mo cob 2/employer GHP
14 MSP, no fault, including auto primary
15 MSP, workmans comp primary
16 MSP, PHS or other Fed agency
41 MSP, black lung
42 MSP, Veteran's Administration (VA)
43 MSP, disabled under 65 with LGHP
47 MSP, other insurance is primary
Employ Status (Employment Status)
Please enter Patient's employment Status
Patient Status
1=Employed
2=Full time student
3=Part time student
4=Leave blank
WorkRelated
Please enter (Y/N) Was this work related?
Other Accident
Please enter (Y/N) Was this related to an accident other than auto?
AutoAccident
Accident related to Auto
Please enter (Y/N) Was this related to an auto accident?
AAPlace
Accident Place
Please enter Auto Accident: PLACE (State)
Box 10d
Please enter data reserved for local use (note Medicare special requirements). If you answer with a dot [.] then you will bring up a menu of possible choices required by Medicare or you may enter what you want to print in box 10d.
Box 10d
1=MSP (4,7,11)
2=2MSP (4,7,11,At)
3=MG (9,9a-9d)
4=MSP/MG (4,7,11,At) / (9,9a-9d)
5=2MSP/MG (4,7,11,At) / (9,9a-9d)
6=MSP/MG/SP (4,7,11,At) / (9,9a-9d)
7=SP (9,9a-9d)
8=MSP/SP (4,7,11,At) / (9,9a-9d)
9=MG/SP (9,9a-9d) / (At)
A=MCD (9,9a,9b)
B=MSP/MCD (4,7,11 add:9c,9d / (9,9a,9b)
C=MG/MCD (9,9a-9d) / (11,11a)
D=MSP/MG/MCD (4,7,11 add:At) / (9,9a-9d) / (At)
Leave Box 10d Blank (CMS 12/90 form)
Box 11d
Please enter
1 Yes, there is another plan
2. No, there is not another plan
3 Leave blank
4 use the defaults
PaperWrkType
Right-click will give you many choices for the qualifier code and the meaning.
PaperWrkSent
Right-click will give you many choices for the qualifier code and the meaning.
FamilyPlan
Family Planning
Please enter (Y/N) Is this related to family planning?
PrAuthNo
Preauthorization Number
Please enter the preauthorization number.
EPSDT
Please enter (Y/N) is this related to EPSDT
Entering a New Referrer Name
See Add a new Referring Person
SSI® Note: You must have the NPI code for all providers.
Entering a Supervising Name
See Add a new Supervising Person
Entering a New Facility Name
See Add a new Facility
Entering a New Laboratory Name
See Add a New Laboratory
Dt Hosp From
Date Hospitalization, Begin
Please enter the date the hospitalization began
Dt Hosp To
Date Hospitalization, End
Please enter the date the hospitalization ended.
Dt Totl Disability From
Date Total Disability, Begin
Please enter the date the total disability began.
Dt Totl Disability To
Date Total Disability, End
Please enter the date the total disability ended.
Dt Illness Began
Date of Illness, (beginning date)
Please enter the date the illness began.
Dt Sim Symptom
Date Similar Illness, (beginning date)
Please enter the date the similar symptoms began.
And others.
We hope the labels are self explanatory. If not, please contact support. You could suggest a better label or a 'tool tip text'